Menu
Close
Menu
Paediatric occupational therapy is dedicated to nurturing children’s skills for functional independence, fostering their growth into confident individuals. Through targeted interventions, we support children in overcoming challenges across physical, social, and cognitive development stages, guiding them towards maturity with strength and assurance.
Our pediatric occupational therapists specialize in working with children and adolescents facing various conditions or disabilities that hinder their participation in daily tasks. Employing an integrative client-centered approach, we offer practical solutions to enhance participation, independence, and engagement in all aspects of a child’s life. Our goal is to empower children to achieve maximum independence promptly, benefiting both them and their parents.
Through comprehensive evaluation and targeted interventions, our paediatric occupational therapists strive to support children in achieving their full potential and thriving in their daily lives.


The occupational therapist, in conjunction with other practitioners, work together with the client to focus on individual and environmental abilities and problems related to activities in the person’s daily life.

The results of the assessment are the basis of the plan which includes short and long-term aims of treatment. The plan should be relevant to the person’s development stage, habits, roles, life-style preferences and the environment.

Intervention focuses on programs that are person oriented and environmental. These are designed to facilitate the performance of everyday tasks and adaptation of settings in which the person works, lives and socialises.
Involves utilising objects within the hand such as cutlery or pencils for play, self-care and handwriting skills.
Are those that are used in everyday play, such as threading and using puzzles as well as the imaginative, social and communication requirements such as turn taking, sharing, winning/losing.
Involve skills such as feeding, dressing, bathing, grooming, sleeping and toileting.
Through comprehensive evaluation and targeted interventions, we strive to support children in achieving their full potential and thriving in their daily lives.

Physiotherapists focused on paediatric physiotherapy collaborate with children and their families to identify movement and functional challenges. Our goal is to assist children in managing their physical symptoms and attaining functional mobility. Through assessment, treatment, and guidance, we empower children to engage in exercises and activities both at home and in educational settings.
Our paediatric physiotherapy service caters to a broad spectrum of conditions, including Autism Spectral Disorder, developmental motor skill delays, musculoskeletal issues, cerebral palsy, and various neuromuscular conditions. Utilizing play, activities, and tailored exercise regimes, we endeavor to support children in realizing their full physical potential.
Central to our approach is the education of families and caregivers about the child’s condition, alongside implementing a structured program of activities aimed at skill maintenance or development. Collaboration with parents and educational professionals is paramount, and we frequently liaise with other healthcare, educational, and social care experts to ensure comprehensive support for the child’s holistic well-being.
Dr. Arini Verwer, PhD, developed Social Brain & Interaction protocols, which focus on brain development and the influence of the social environment on emotional state and behaviour. This therapy aims to assist families in understanding each family member’s emotional needs through communicative patterns of behavior and movement. Social Brain therapy is grounded in the science of learning and behavior, pinpointing a child’s learning style, emotional needs, and value system that drive behavior. Through parent coaching services, specific tools and skills are identified and applied to help the child in everyday life, fostering emotional regulation, independence, and improved social interaction.




Using state-of-the-art technology, we employ Quantitative Electroencephalography (QEEG) brain mapping to create brain maps, which illustrate the electrical activity of the brain. This is then statistically compared to a database of ‘normal’ brain activity, providing a quantitative indication of the differences in brain function from normal. The functional Brainwave patterns so revealed can indicate the underlying brain physiology that may be associated with certain dysfunctional conditions, as well as the severity of the condition.
Our QEEG analysis is independently analysed by an expert team , using several Analysis systems, examples of which are shown below. A report is returned to us with an explanation of findings and recommendations for Neurofeedback training.
Neurofeedback (also called Neurotherapy or EEG biofeedback) is, in essence, a way of training the brain to use more productive patterns of brainwaves. It is a non-invasive treatment, that teaches the brain to self-regulate, strengthening neural pathways while increasing mental endurance and flexibility.
Neurotherapy is accompanied by functional brain exercises, treatments, and Nutritional supplementation to optimise brain health.
“…parents interested in non-psycho pharmacologic treatment can pursue the use of complementary and alternative therapy. The therapy most promising by recent clinical trials appears to be EEG biofeedback.”
Dr. Katie Campbel Daley
Harvard Medical School
One of the most important building blocks for achieving health, wealth, and vitality resides in the healing powers of sleep. Sleep is food for the brain, get enough of it and get it when you need it. After oxygen and water, sleep is the most important need, even more important than food.
Sleep is divided into 4 stages Non-REM 75% (purple) sleep and REM (Blue) 25% sleep (Rapid Eye Movement). These are sometimes referred to as “sleep phases” or “sleep cycles“.
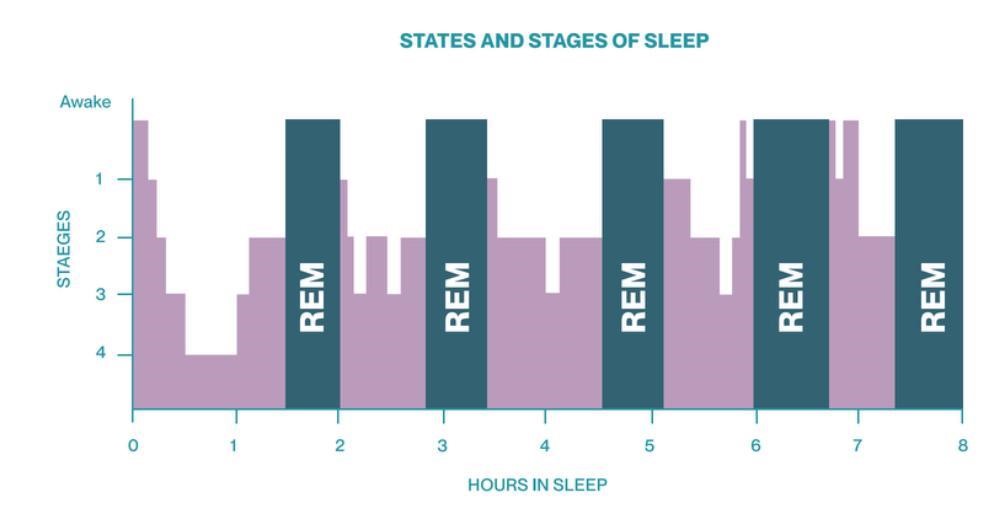
Non REM is responsible for regeneration, detoxification ( liver, Non-REMgut, lymphatic system), repair, & hormonal regulation.
REM sleep is responsible for emotional regulation, memory reconsolidation & learning.
Dreaming occurs in both stages but mostly during REM sleep. Each cycle of NREM and REM is repeated every 90 minutes, 4 to 5 times a night. 5-6 cycles is an ideal amount of sleep required for everyone after 15 years old.
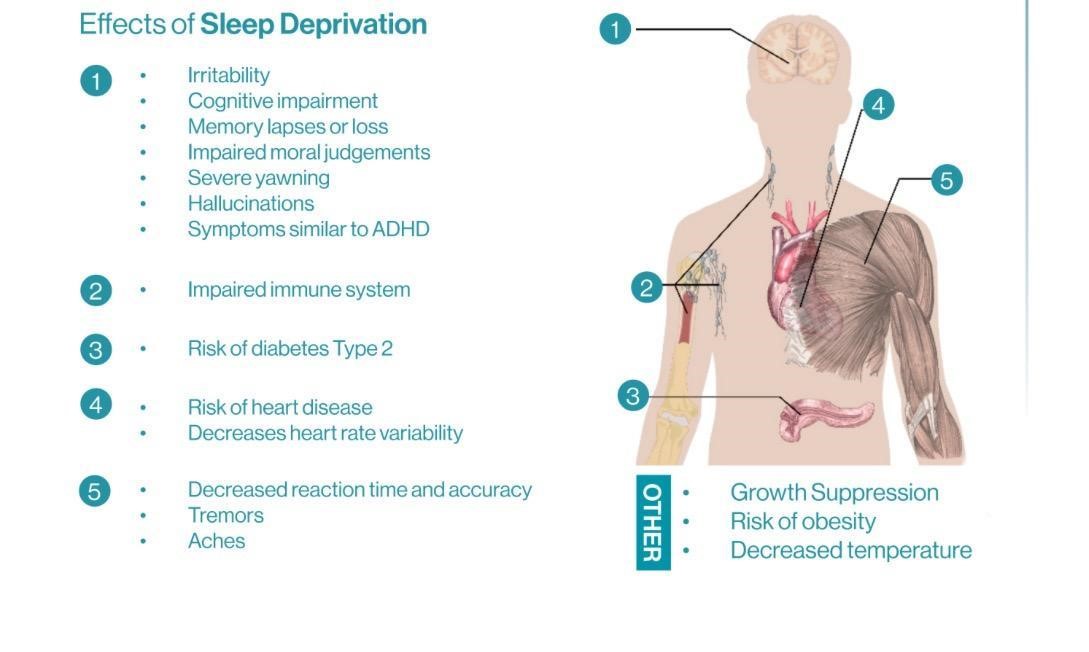
Sleep is necessary for detoxification, immunity, tissue repair, regeneration, memory consolidation, learning, emotional balancing, and most importantly for recuperation of the brain from the day’s activities.
When we achieve quality sleep, we prime the emotional brain properly; balancing brain chemicals and creating a positive and energetic state of mind. The result is a feeling of mental and physical energy and an internal psychological push called motivation. Without it, we may get depressed and sick.
Sleep disturbances have been found to negatively affect behavior, cognition, and growth, areas that are also the focus of early intervention efforts. Conversely, developmental delays and disabilities themselves can contribute to the occurrence of sleep disorders. Among young children, those with developmental delays exhibit a higher prevalence of sleep disorders compared to their typically developing peers, with difficulties initiating or maintaining sleep and sleep disordered breathing being the most common types. While previous research has primarily concentrated on sleep issues in children with specific conditions such as autism, genetic syndromes, prematurity, and seizure disorder, this article aims to explore the broader impact of sleep problems across all children who undergo screening for early intervention services.



Children with autism and developmental delay exhibit impairments in social interaction and display repetitive patterns of behavior. Autism encompasses a diverse range of disorders with an unknown etiology. Research in this field has expanded significantly, suggesting that environmental risk factors acting during the prenatal period could influence offspring neurodevelopment. The literature indicates that maternal diet during pregnancy plays a fundamental role in the etiopathogenesis of autism. Indeed, a maternal diet high in certain nutrients has been associated with either an increase or reduction in the risk of developing Autism Spectrum Disorders (ASD). Additionally, the dietary habits of children with ASD are crucial factors that can impact the severity of ASD symptoms. These children often exhibit food selectivity and limited diets due to sensitivities related to smell, taste, or other characteristics of foods. As a result, their eating routines and food intake patterns may lead to deficiencies or excesses of certain nutrients. Several studies have attempted to explore the potential relationship between nutritional status and autism.
Following a metabolic assessment, we assist parents in implementing a tailored dietary program that best suits the child’s needs.

DIR Floortime
DIR Floortime is about making the child feel safe. The Developmental, Individual-differences, & Relationship-based (DIR) model, pioneered by Dr. Stanley Greenspan, serves as a foundational framework for comprehending human development. Emphasizing the crucial role of social-emotional development from birth onward, the model elucidates how individuals perceive and interact with the world uniquely. Central to the DIR model is the recognition of relationships and emotional connections as catalysts for development.
While the DIR training facilitates understanding and fosters positive development in all children, it is primarily employed with those facing educational, social-emotional, mental health, and developmental challenges. Notably, DIR/Floortime, an offshoot of the DIR model, is widely recognized for its effectiveness in supporting children with Autism Spectrum Disorders (ASD).
Dr. Arini Verwer, PhD, developed Social Brain & Interaction protocols, which focus on brain development and the influence of the social environment on emotional state and behaviour. This therapy aims to assist families in understanding each family member’s emotional needs through communicative patterns of behavior and movement. Social Brain therapy is grounded in the science of learning and behavior, pinpointing a child’s learning style, emotional needs, and value system that drive behavior. Through parental coaching, specific tools and skills are identified and applied to help the child in everyday life, fostering emotional regulation, independence, and improved social interaction.
The program aims to assist individuals in our community facing neurodevelopmental disorders, such as Autism spectrum disorders, Asperger’s, ADHD, Dyslexia, Processing disorders, Sensory processing disorders, Developmental delay, and Poor social skills. It integrates practices from functional neurology, occupational therapy, vision therapy, and cutting-edge digital technology, currently being patented as digital medicine.

It is notable that areas of the brain involved in movement, such as the Cerebellum, Basal Ganglion, Thalamus, and prefrontal cortex, also play roles in cognition and emotional integration. These areas have motor and non-motor functions that collaborate to modulate cognition, emotional behavior, and movement.
Muscular activities pattern themselves during the development of primitive reflexes (fixed action patterns) as they adapt to gravity. The Cerebellum, vestibular system, limbic system (Basal ganglion, Thalamus), and prefrontal cortex serve as the control center for these movement patterns, influenced by chemical and structural stress, as well as the individual’s emotional state.
If these reflexes persist beyond their typical time span, they are considered aberrant, retained, and indicative of structural weakness or immaturity within the central nervous system. The integration and inhibition of primitive reflexes are crucial for maintaining brain energy efficiency.
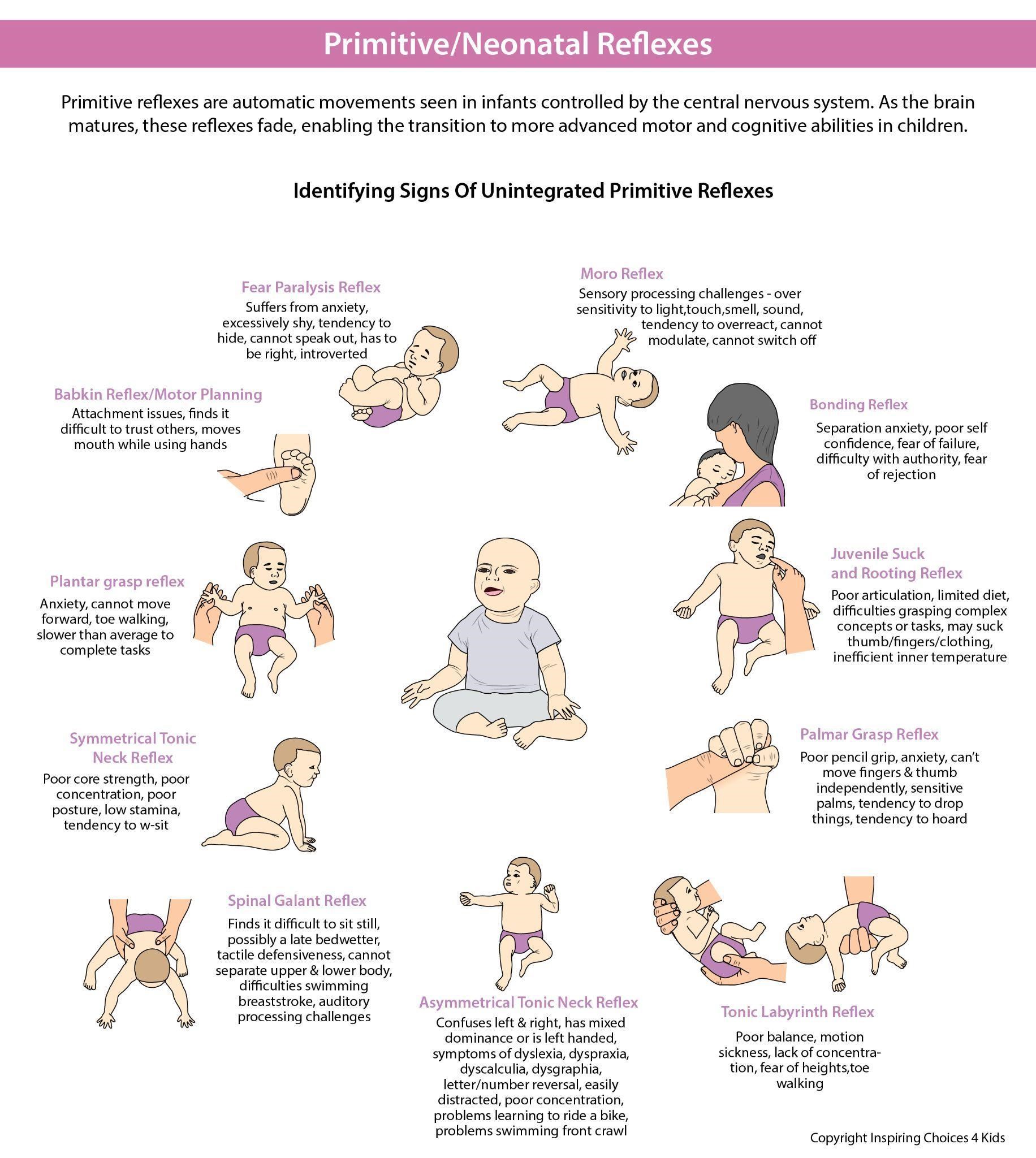
Primitive reflexes emerge in utero, are present at birth, and typically are inhibited by 6-12 months of age. Reflex inhibition correlates with control by higher brain centers, facilitating the development of more complex neural structures and voluntary movements.
These fixed motor patterns give rise to goal-oriented movements and proper development of the neocortex. Delay or disruption in this bottom-up projection, termed “bottom-up interference,” can delay the development of more advanced brain areas, potentially hindering top-down maturational processes that inhibit these reflexes.
Retained primitive reflexes can also impact a child’s sensory perceptions, causing hypersensitivity or hyposensitivity and contributing to asymmetry in left and right brain information processing, speed, and timing.
Emotions can be viewed as a form of fixed action pattern, considered premotor in nature. Just as muscle tone serves as a base platform for muscle movement, emotions serve as premotor platforms that either drive or deter actions. For example, children with autistic spectrum disorders and attention deficit hyperactive disorders may exhibit stereotyped movement patterns due to uninhibited fixed action patterns, resembling hyperkinetic movements.
Some of the modalities utilized in the implementation of our Neuro Rehab and cognitive therapy protocol based on your child’s needs and evidence available for their use are:
Pitcher TM, Piek JP, Hay DA. Fine and gross motor ability in males with ADHD. Dev Med Child Neurol. 2003 Aug;45(8):525-35.
Foulder-Hughes LA, Cooke RW. Motor, cognitive, and behavioural disorders in children born very preterm. Dev Med Child Neurol. 2003Feb;45(2):97-103.
Goddard S, A Teacher’s window into the Child’s Mind, Fern Ridge Press 1996 :P1-4
Connectivity in Autism Spectrum Disorders
by Robert Melillo 1,Gerry Leisman 1,2,*,Calixto Machado 3,Yanin Machado-Ferrer 3,Mauricio Chinchilla-Acosta 3,Ty Melillo 4 andEli Carmeli 1
Brain Sci. 2023, 13(8), 1147; https://doi.org/10.3390/brainsci13081147
McPartland, J.; Volkmar, F.R. Autism and related disorders. Handb. Clin. Neurol. 2012, 106, 407–418.
Gabard-Durnam, L.; Tierney, A.L.; Vogel-Farley, V.; Tager-Flusberg, H.; Nelson, C.A. Alpha Asymmetry in Infants at Risk for Autism Spectrum Disorders. J. Autism Dev. Disord. 2015, 45, 473–480. [Google Scholar] [CrossRef] [Green Version]
Cognitive Rehabilitation in Developmental Disabilities.
https://www.drrobertmelillo.com/research/2015-Machado-Leisman-BainConnectivity.pdf
QEEG Spectral and Coherence Assessment of Autistic Children in Three Different Experimental Conditions, Calixto Machado • Mario Este´vez • Gerry Leisman • Robert Melillo • Rafael Rodrı´guez • Phillip DeFina • Adria´n Herna´ndez • Jesu´s Pe´rez-Nellar • Rolando Naranjo • Mauricio Chinchilla • Nicola´s Garo´falo • Jose´ Vargas • Carlos Beltra´n
Journal of Autism and Developmental Disorders ISSN 0162-3257 Volume 45 Number 2 J Autism Dev Disord (2015) 45:406-424 DOI 10.1007/s10803-013-1909-5
Effects of Music Training and Production on Functional Brain Organization – 2012
Autistic Spectrum Disorders as Functional Disconnection Syndrome, Robert Melillo1 and Gerry Leisman, Rev Neurosci 2009; 20(2):111-3
Dev Med Child Neurol. 2003 Aug;45(8):525-35. Pitcher TM, Piek JP, Hay DA
Dev Med Child Neurol. 2003 Feb;45(2):97-103.Foulder-Hughes LA, Cooke RW.
Fern Ridge Press 1996 :P1-4. Goddard S,
by Robert Melillo 1,Gerry Leisman 1,2,*,Calixto Machado 3,Yanin Machado-Ferrer 3,Mauricio Chinchilla-Acosta 3,Ty Melillo 4 andEli Carmeli 1
Robert Melillo, Gerry Leisman, Calixto Machado, Yanin Machado-Ferrer, Mauricio Chinchilla-Acosta, Ty Melillo, and Eli Carmeli.
Brain Sci. 2023, 13(8), 1147
1 Movement and Cognition Laboratory, Department of Physical Therapy, University of Haifa, Haifa 3498838, Israel
Handb. Clin. Neurol. 2012, 106, 407–418.
McPartland, J.; Volkmar, F.R.
Gabard-Durnam, L Tierney, A.L.; Vogel-Farley, V.; Tager-Flusberg, H.; Nelson, C.A. J. Autism Dev. Disord. 2015, 45, 473–480.
1,2,*,Robert Melillo 1,Ty Melillo 3,Calixto Machado 4,Yanin Machado-Ferrer 4,Mauricio Chinchilla 4 andEli Carmeli .Symmetry 2022, 14(12), 2689;
Calixto Machado,1 Rafael Rodrı´guez,2 Mario Este´ vez,1 Gerry Leisman,3–5 Robert Melillo,6 Mauricio Chinchilla,1 and Liana Portela1
https://www.drrobertmelillo.com/research/2015-Machado-Leisman-BainConnectivity.pdf
Calixto Machado • Mario Este´vez • Gerry Leisman • Robert Melillo • Rafael Rodrı´guez • Phillip DeFina • Adria´n Herna´ndez • Jesu´s Pe´rez-Nellar • Rolando Naranjo • Mauricio Chinchilla • Nicola´s Garo´falo • Jose´ Vargas • Carlos Beltra´n
ISSN 0162-3257 Volume 45 Number 2 J Autism Dev Disord (2015) 45:406-424 DOI 10.1007/s10803-013-1909-5
Effects of Music Training and Production on Functional Brain Organization – 2012
Robert Melillo1 and Gerry Leisman, Rev Neurosci 2009; 20(2):111-31
If you have a general inquiry that is not time-sensitive, fill out the Contact form or contact us via the details below and one of our team will get back to you. We are open daily 9:00 am – 5:00 pm Monday to Friday (excluding public holidays).
+61 (07) 5575 7281
info@inspiringchoices4kids.com.au
Suite 1 & 3, 328 Scottsdale Drive,Robina Gold Coast, QLD 4226
